
Lay Summary
POMT2-CDG is a rare inherited condition that affects many parts of the body. To date, there are at least 40 patients reported in the medical literature. POMT2-CDG is classified as a disorder of O-linked protein glycosylation and more specifically, a disorder of O-mannosylation. POMT2-CDG is also classified as a dystroglycanopathy, which refers to a group disorders that affect the glycosylation of the protein alpha-dystroglycan. The alpha-dystroglycan protein plays an important role in muscle, brain and eye development. POMT2-CDG is caused when an individual has mutations in both copies of their POMT2 gene, which encodes an enzyme that attaches the simple sugar mannose to a protein during O-glycosylation. Mutations in the POMT2 gene cause proteins to be under glycosylated, meaning these proteins have less sugars attached than healthy forms of the proteins. POMT2-CDG can present as three different forms that range in severity, with symptoms beginning from birth or in adolescence depending on the form. POMT2-CDG is primarily characterized by muscle, brain, eye, and heart problems. Screening tests are available for POMT2-CDG, but a definitive diagnosis is achieved through genetic testing. Treatment is focused on the management of specific symptoms and preventing complications.
Overview
Protein O-mannosyltransferase 2 congenital disorder of glycosylation (POMT2-CDG) is a rare autosome recessive genetic disorder. The first case of POMT2-CDG was reported in 2005, and there are at least 40 reported cases in the literature to date1–9. The POMT2 gene encodes an enzyme, protein O-mannosyltransferase 2 (POMT2), which is responsible for adding the first mannose to serine or threonine residues on a protein during O-glycosylation10. Deficiency of POMT2 results in deficient O-mannosylation of the protein alpha-dytroglycan – a protein that is part of the dystrophin-glycoprotein complex that is needed for a range of roles, such as stabilizing muscle tissue and cell signalling5. POMT2-CDG is also classified as a dytroglycanopathy, which refers to a group of disorders that affect O-mannosylation of alpha-dystroglycan.
POMT2-CDG may present as three different forms; Muscular dystrophy-dystroglycanopathy type A2, -type B2 or -type C2, which vary in clinical presentation and symptom severity. The characteristic clinical presentation of POMT2-CDG includes muscle, brain, and eye problems. Definitive diagnosis can only be achieved through molecular genetic testing. There are currently no approved treatments for POMT2-CDG.
Synonyms
- Muscular dystrophy-dystroglycanopathy, type A2 (MDDGA2), WWS, MEB
- Muscular dystrophy-dystroglycanopathy, type B2 (MDDGB2), CDM-ID
- Muscular dystrophy-dystroglycanopathy, type C2 (MDDGC2), LMGD 2N
- O-Mannosyltransferase 2 deficiency
Inheritance
POMT2-CDG is inherited in an autosomal recessive fashion, where a mutation is inherited from each parent (asymptomatic carriers).
Gene Function
POMT2 encodes a mannosyltransferase enzyme, protein O-mannosyltransferase 2 (POMT2). Mannosyltransferases are enzymes that enable the transfer of mannose during glycosylation. POMT2 is located in the ER membrane, with exposed sections in the cytoplasm and the ER lumen. POMT2 adds mannose to a serine or threonine amino acid residue of a protein during O-glycosylation in the ER. POMT2 must form a complex with a separate enzyme, O-mannosyltransferase 1 (POMT1), to transfer mannose to a protein10. Alpha-dystroglycan is an O-mannosylated protein that has been reported to be abnormally glycosylated in POMT2-CDG patients.
O-mannosylation of alpha-dystroglycan
Alpha-dystroglycan is an O-mannosylated glycoprotein that is found on various cells, such as muscle, heart, and nerve11. O-mannosylation is a type of O-glycosylation which involved the attachment of mannose to serine or threonine residues on a protein. Alpha-dystroglycan is the central component of the dystrophin-glycoprotein complex, which links the extracellular matrix to the intracellular cytoskeleton of muscle cells. Glycosylated alpha-dystroglycan binds to components of the extracellular matrix, such as laminin, and to beta-dystroglycan—which is a protein that is in the cell membrane that joins to the intracellular protein dystrophin12. Alpha-dystroglycan needs to be O-glycosylated to bind to laminin. Alpha-dystroglycan is also needed for a variety of other processes, such as development and cell signalling12,13.
Alpha-dystroglycan O-glycans can have variable structures, where different tissues can have alpha-dystroglycan with different O-glycans. The o-mannosylated glycans on alpha-dystroglycan can be categorized into three core structures – M1, M2, and M3 – which can then be further modified (Figure 1)14.
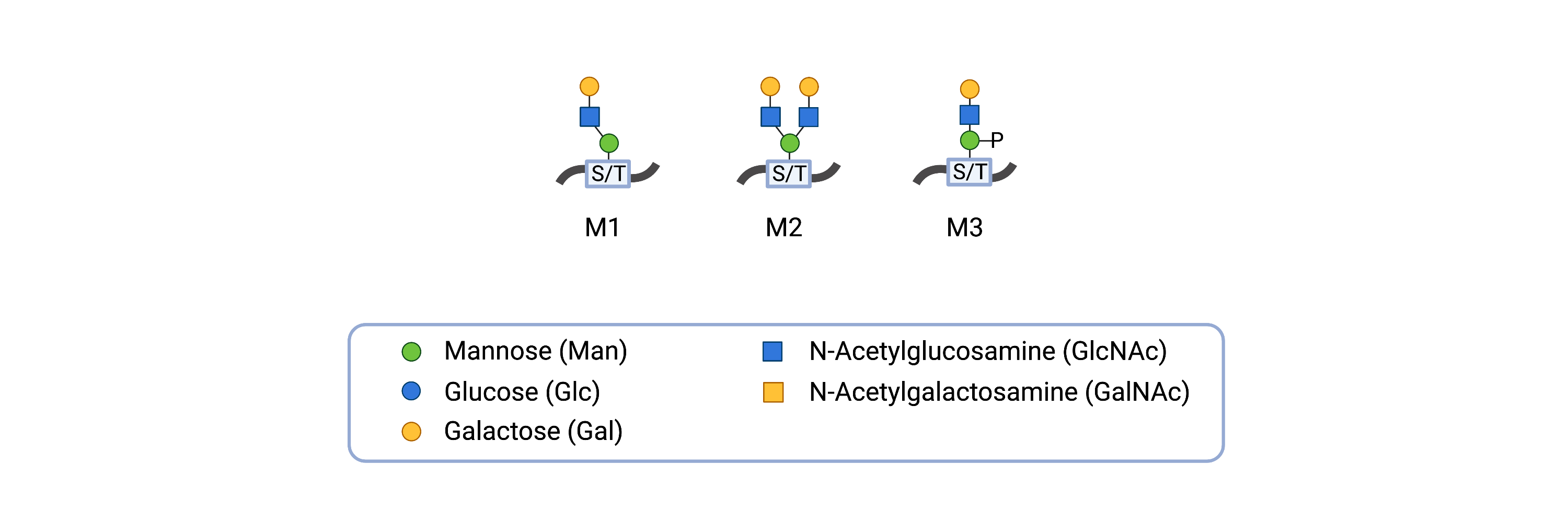
Figure 1.O-mannosyl glycan core structures of alpha-dystroglycan.
The o-mannosylated glycans on alpha-dystroglycan can be categorized as cores M1, M2, or M3 and can be extended by the attachment of additional monosaccharides to the glycan.
However, the first step of O-mannosylation of alpha-dystroglycan requires an initial mannose to be added to the protein. For this, the enzyme complex comprised of POMT1 and POMT2, catalyze the transfer of a single mannose resiude from dolichol-phosphate mannose (Dol-P-Man) to a serine or threonine residue on alpha-dystroglycan in the ER10. Depending on the final structure, additional enzymes modify the O-glycan in the ER and/or Golgi (Figure 2)15.
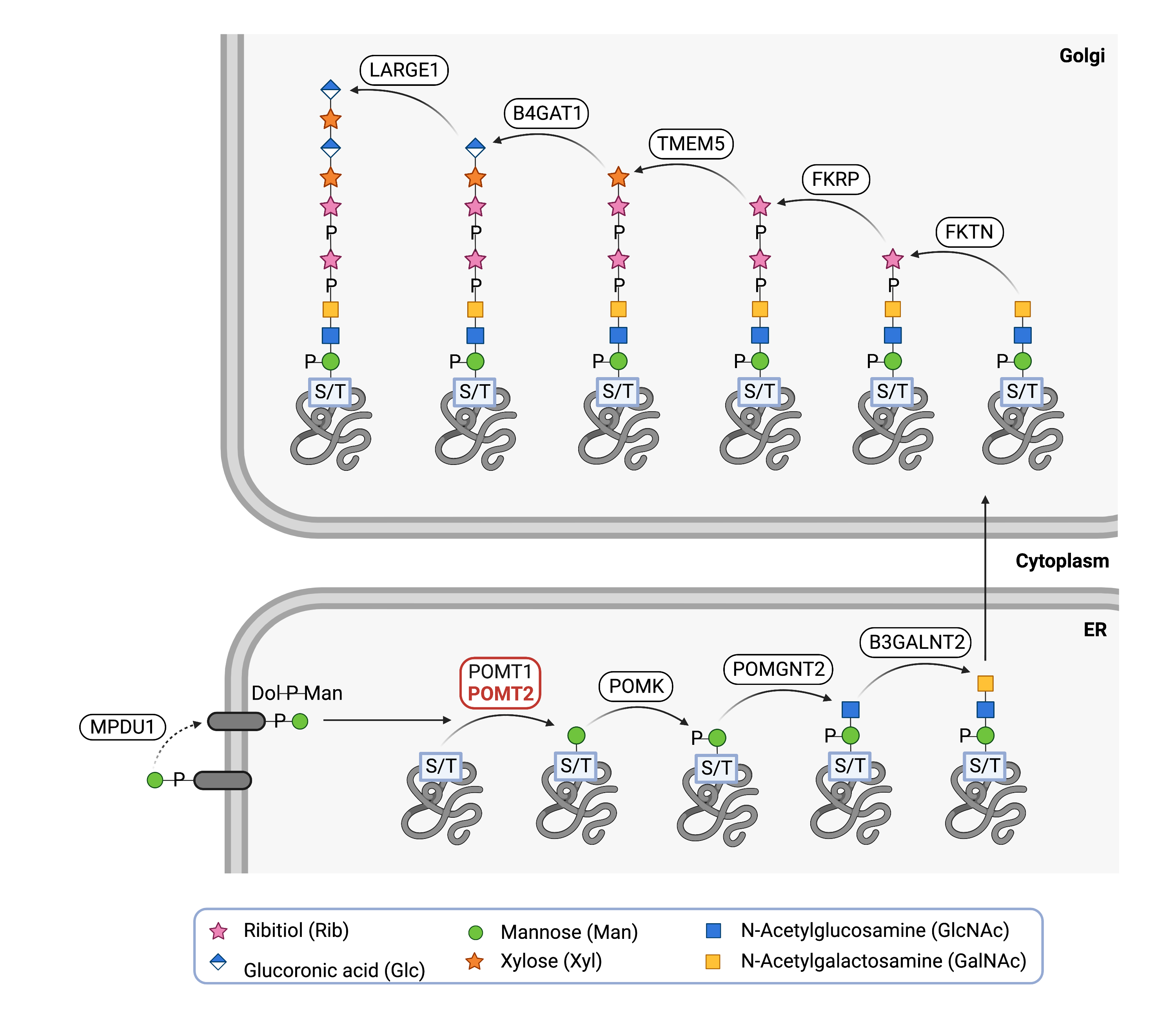
Figure 2.Role of POMT2 in O-mannosylation of alpha-dystroglycan.
POMT2, along with POMT1, attaches the first mannose in the glycan chain to a serine or threonine residue of a protein, such as alpha-dystroglycan. Additional enzymes attach subsequent monosaccharides to generate the glycan chain on alpha-dystroglycan.
Disease Mechanism
Mutations in the POMT2 gene lead to POMT2 having a reduced ability or inability to transfer mannose onto a protein during O-glycosylation. Dystroglycan (DG) is an important cell membrane glycoprotein, linking cytoskeleton of muscles and nerve cells to the extracellular matrix. α-DG is one of two subunits that is post-translationally cleaved from DG, which is O-mannosylated by POMT1 and POMT2. Hypoglycosylation of α-DG prevents the protein from functioning properly and leading to clinical features such as muscle, nerve, and eye problems observed in POMT2-CDG5.
Mutations
The POMT2 gene is located on chromosome 14 (14q24.3). At least 36 pathogenic mutations have been reported for the POMT2 gene, the majority being missense mutations 2,16. The various phenotypes of POMT2-CDG are linked to the level of POMT2 activity. The more severe phenotype like Walker-Warburg syndrome is associated with nonsense mutations and splice site mutations, disrupting an important restriction site in the gene17.
Signs & Symptoms
Clinical Presentation
Muscular dystrophy-dystroglycanopathy (congenital with brain and eye anomalies) type A2; MDDGA2
MDDGA2 is a severe form of congenital muscular dystrophy-dystroglycanopathy, typically presenting prenatally or at birth with brain and eye defects. It includes disorders such as Walker-Warburg syndrome (WWS) and muscle-eye-brain disease (MEB). The clinical presentation may include a combination of:
- Neurological – profound to severe mental retardation, severe hypotonia, hypoplasia, microcephaly, dysplasia, build-up of fluid in the brain (hydrocephalus), defective brain development, and seizures
- Musculoskeletal – severe hypotonia, muscular dystrophy, muscular hypertrophy, scoliosis, rigid spine
- Ophthalmological – microphthalmia, cataracts, glaucoma, myopia, bupthalmos, hypermetropia
Muscular dystrophy-dystroglycanopathy (congenital with intellectual disability) type B2 ; MDDGB2
MDDGB2 is a moderate severe form of congenital muscular dystrophy-dystroglycanopathy associated with impaired intellectual development and mild structural brain abnormalities. Symptoms typically presenting at birth or in infancy. The clinical presentation of MDDGB2 is milder than MDDGA2; it may include a combination of:
- Neurological – delayed motor development, mental retardation, delayed or lack or speech development, hyporeflexia, areflexia, patients may only achieve sitting or walking, microcephaly
- Musculoskeletal – hypotonia, muscle weakness, muscular dystrophy, muscle hypertrophy, scoliosis
- Ophthalmological – myopia, strabismus
- Cardiovascular – left ventricular abnormalities, dilated aortic root
Muscular dystrophy-dystroglycanopathy (limb-gurdle) type C2; MDDGC2
MDDGC2 is a form of limb-girdle muscular dystrophy presenting with or without intellectual disability. It is also known as limb-gurdle muscular dystrophy type 2N (LGMD2N) and limb-gurdle muscular dystrophy autosomal recessive 14 (LGMDR14). Symptom onset of MDDGC2 occurs after independent walking ability is achieved. The clinical presentation may include a combination of:
- Neurological – delayed motor development
- Musculoskeletal – muscle weakness, muscular dystrophy, muscular hypertrophy
Biochemical Abnormalities
Biochemical abnormalities observed in individuals with POMT2-CDG include elevated serum creatine levels.
Classification
POMT2-CDG is classified as a disorder of O-linked protein glycosylation and within this group, a disorder of O-mannosylation.
Diagnosis
Although diagnosis of POMT2-CDG may be suspected based on the presentation of symptoms and a detailed patient history, direct molecular genetic testing is the only definitive diagnostic test. Screening tests in suspected patients can involve immunostaining of alpha-dystroglycan from muscle cell samples.
Alpha-dystroglycan staining
Muscle biopsies taken from patients are stained or immunolabeled with antibodies that bind to glycosylated alpha-dystroglycan. Consequently, hypoglycosylated alpha-dystroglycan will have lower binding levels and immunolabeling than healthy alpha-dystroglycan16.
Biomarkers
There are currently no biomarkers for POMT2-CDG.
Prognosis
Prognosis of POMT2-CDG may vary depending on the severity of an individual’s symptoms and the form of the disease.
Most severely affected patients (Walker-Warburg syndrome) cannot obtain mobility and do not survive beyond 1-3 years of age. In the case of the second severe form of POMT2-CDG (muscle-eye brain disease), some patients may achieve the ability to walk, but will have language and intellectual disability16.
The mildest form (LGMD type 2N), presents with late onset and mild muscle weakness16. Patients with this form of POMT2-CDG have been reported in live into adulthood, with the oldest patient recorded at 63 years old20.
Management
Management of symptoms may include combinations of physical therapy, occupational therapy, vision therapy, and palliative measures.
Therapies
There are currently no treatment options available for POMT2-CDG. Treatment is focused on the management of symptoms and prevention of complications.
Research Models
Several POMT2 models have been generated, such as in flies, fish, mice, and human cells.
Fly (D. melanogaster)
Drosophila gene dPOMT2 is orthologous to human POMT2. Glycosylation of Dg by POMT1 and POMT2 are important to Dg function in maintaining cell integrity in the muscles of larval Drosophila. Mutations in dPMOT1 in larvae show defects in muscle attachment and contraction in phenotypes with impaired or hypoglycosylated dystroglycan21.
RNAi dPOMT2 mutants show a twisted/rotated abdomen phenotype (rt, tw), similar to dPOMT1 mutant phenotypes22,23. Additionally, mutant flies show abnormalities in motor function, specifically climbing and flight, as well as defects in muscle ultrastructure24.
POMT mutant embryos show a left-handed body torsion phenotype, resulting from aberrant muscle contractions. POMT mutants were found to have defective axonal connections to sensory neurons, suggesting that protein O-mannosylation is required for sensory feedback to control muscle contractions and posture25.
Fish (D. rerio)
The POMT2 orthologue has been identified in zebrafish26.
Mouse (M. musulus)
Pomt2 Expression in Mice
In mice embryos, somatic Pomt2 (sPomt2) but not testis-specific Pomt2 (tPomt2) is predominantly expressed in developing muscle, eye, and brain27.
Homozygous Pomt2-/- Knockout Mice
Homozygous Pomt2 knockout mice were found to be embryonic lethal 28.
Pomt2 Brain-specific Conditional Knockout Mice
Brain-specific knockout of Pomt2 in mice resulted in hypoglycosylation of alpha-dystroglycan and eliminated laminin binding activity. Deletions earlier in brain development were also found to have a more severe phenotype28.
Human Cell Lines
Human Embryonic Kidney Stem Cells (HEK293T)
Plasmids with POMT1 and POMT2 transfected into HEK293T cells showed that POMT1 and POMT2 must be co-expressed to form an active enzyme complex29.
Clinical Studies
Active
Clinical and Basic Investigations into Congenital Disorders of Glycosylation (NCT04199000)
The Frontiers in Congenital Disorder of Glycosylation Disorders Consortium (FCDGC) is conducting a 5-year natural history study on all CDG types, including POMT2-CDG. The purpose of this study is to define the natural history and clinical symptoms of CDGs, develop new diagnostic techniques, identify clinical biomarkers that can be used in future clinical trials and evaluate whether dietary treatments improve clinical symptoms and quality of life.
Publications
POMT2-CDG Scientific Articles on PubMed
Additional Resources
OMIM - MDDGA2
OMIM - MDDGB2
OMIM - MDDGC2
IEMbase
MedlinePlus
Orphanet
Genetic Testing Registry
ClinVar
NIH
GeneCards
UniProt
Marrvel
References
- van Reeuwijk, J. et al. POMT2 mutations cause α-dystroglycan hypoglycosylation and Walker-Warburg syndrome. Journal of Medical Genetics 42, 907 (2005).
- Messina, S. et al. POMT1 and POMT2 mutations in CMD patients: a multicentric Italian study. Neuromuscul Disord18, 565–571 (2008).
- Biancheri, R. et al. POMT2 gene mutation in limb-girdle muscular dystrophy with inflammatory changes. Biochem Biophys Res Commun 363, 1033–1037 (2007).
- Gan, S., Yang, H., Xiao, T., Pan, Z. & Wu, L. POMT1 and POMT2 gene mutations result in 2 cases of alpha- dystroglycanopathy. Zhong Nan Da Xue Xue Bao Yi Xue Ban 46, 915–919 (2021).
- Mahjoub, G., Faghihi, M. A. & Taghdiri, M. Reporting one very rare pathogenic variation c.1106G>A in POMT2 gene. Intractable & Rare Diseases Research 9, 104 (2020).
- Yıldırım, M., Eker, H. K. & Doğan, M. T. A homozygous mutation in the POMT2 gene in four siblings with limb-girdle muscular dystrophy 2N. Turkish Archives of Pediatrics 56, 68 (2021).
- Messina, S. et al. POMT1 and POMT2 mutations in CMD patients: a multicentric Italian study. Neuromuscul Disord18, 565–571 (2008).
- Yanagisawa, A. et al. New POMT2 mutations causing congenital muscular dystrophy: identification of a founder mutation. Neurology 69, 1254–60 (2007).
- Martinez, H. R. et al. Novel cardiovascular findings in association with a POMT2 mutation: three siblings with α-dystroglycanopathy. European Journal of Human Genetics 2014 22:4 22, 486–491 (2013).
- Akasaka-Manya, K., Manya, H., Nakajima, A., Kawakita, M. & Endo, T. Physical and functional association of human protein O-mannosyltransferases 1 and 2. Journal of Biological Chemistry 281, (2006).
- Hewitt, J. E. Abnormal glycosylation of dystroglycan in human genetic disease. Biochimica et Biophysica Acta - Molecular Basis of Disease vol. 1792 Preprint at https://doi.org/10.1016/j.bbadis.2009.06.003 (2009).
- Endo, T. Glycobiology of alpha-dystroglycan and muscular dystrophy. Journal of Biochemistry 157, (2015).
- Balci-Hayta, B., Talim, B., Kale, G. & Dincer, P. LARGE expression in different types of muscular dystrophies other than dystroglycanopathy. BMC Neurology 18, (2018).
- Yoshida-Moriguchi, T. & Campbell, K. P. Matriglycan: A novel polysaccharide that links dystroglycan to the basement membrane. Glycobiology vol. 25 Preprint at https://doi.org/10.1093/glycob/cwv021 (2014).
- Praissman, J. L. et al. The functional O-mannose glycan on α-dystroglycan contains a phospho-ribitol primed for matriglycan addition. Elife 5, (2016).
- Chen, X. Y. et al. Phenotype and Genotype Study of Chinese POMT2-Related α-Dystroglycanopathy. Frontiers in Genetics 12, 1399 (2021).
- Entry - *607439 - PROTEIN O-MANNOSYLTRANSFERASE 2; POMT2 - OMIM. https://omim.org/entry/607439.
- Clinical Synopsis Table - #613150, #613156, #613158 - OMIM. https://omim.org/clinicalSynopsis/table?mimNumber=613150,613156,613158.
- Muntoni, F., Torelli, S. & Brockington, M. Muscular Dystrophies Due to Glycosylation Defects.
- Østergaard, S. T. et al. Limb girdle muscular dystrophy due to mutations in POMT2. J Neurol Neurosurg Psychiatry89, 506–512 (2018).
- Haines, N., Seabrooke, S. & Stewart, B. A. Dystroglycan and protein O-mannosyltransferases 1 and 2 are required to maintain integrity of Drosophila larval muscles. Molecular Biology of the Cell 18, (2007).
- Martín-Blanco, E. & García-Bellido, A. Mutations in the rotated abdomen locus affect muscle development and reveal an intrinsic asymmetry in Drosophila. Proc Natl Acad Sci U S A 93, 6048–6052 (1996).
- Ichimiya, T. et al. The Twisted Abdomen Phenotype of Drosophila POMT1 and POMT2 Mutants Coincides with Their Heterophilic Protein O-Mannosyltransferase Activity *. Journal of Biological Chemistry 279, 42638–42647 (2004).
- Ueyama, M. et al. Increased Apoptosis of Myoblasts in Drosophila Model for the Walker-Warburg Syndrome. PLOS ONE 5, e11557 (2010).
- Baker, R. et al. Protein O-Mannosyltransferases Affect Sensory Axon Wiring and Dynamic Chirality of Body Posture in the Drosophila Embryo. Journal of Neuroscience 38, 1850–1865 (2018).
- Moore, C. J., Goh, H. T. & Hewitt, J. E. Genes required for functional glycosylation of dystroglycan are conserved in zebrafish. Genomics 92, (2008).
- Lommel, M., Willer, T. & Strahl, S. POMT2, a key enzyme in Walker-Warburg syndrome: somatic sPOMT2, but not testis-specific tPOMT2, is crucial for mannosyltransferase activity in vivo. Glycobiology 18, 615–625 (2008).
- Hu, H. et al. Conditional Knockout of Protein O-mannosyltransferase 2 Reveals Tissue-Specific Roles of O-mannosyl Glycosylation in Brain Development. J Comp Neurol 519, 1320 (2011).
- Manya, H. et al. Demonstration of mammalian protein O-mannosyltransferase activity: Coexpression of POMT1 and POMT2 required for enzymatic activity. Proc Natl Acad Sci U S A 101, (2004).