
Lay Summary
ALG12-CDG, formerly known as CDG-Ig, is a rare inherited condition that affects many systems in the body. To date, there are 16 patients reported in the literature with ALG12-CDG. ALG12-CDG is classified as a disorder of N-linked protein glycosylation. ALG12-CDG is caused when an individual has mutations in both copies of the ALG12 gene, which provides instructions for making an enzyme that attaches the sugar mannose to growing sugar chains during N-glycosylation. Mutations in the ALG12 gene cause proteins to have incomplete or absent sugar chains. Symptoms of ALG12-CDG begin in infancy and are primarily characterized by intellectual disability, low muscle tone, dysmorphic features, low immunoglobulin levels and recurrent infections, and male genital abnormalities. Several screening tests are available for ALG12-CDG, but a definitive diagnosis is achieved through genetic testing. Treatment is focused on the management of specific symptoms and preventing complications.
Overview
Alpha-1,6-mannosyltransferase congenital disorder of glycosylation (ALG12-CDG) is a rare autosomal recessive genetic disorder. The first reported case of ALG12-CDG was in 20021 and there are 16 patients reported to date1–13. The ALG12 (asparagine-linked glycosylation 12) gene encodes a mannosyltransferase enzyme responsible for adding the eighth of nine mannose residues during synthesis of the lipid-linked oligosaccharide (LLO) in the lumen of the endoplasmic reticulum (ER)5. The synthesis of the LLO is a precursor step to N-glycosylation, which is the process by which sugar chains (glycans) are added to the amino acid asparagine in proteins. Deficiency in the ALG12 enzyme results in the incomplete assembly of N-glycans, leading to insufficient glycosylation of glycoproteins5.
Symptoms begin in infancy and the characteristic presentations of ALG12-CDG include intellectual disability, low muscle tone, dysmorphic features, low immunogloublin levels with recurrent infections, male genital abnormalities, and coagulation abnormalities5. A diagnosis can be determined through transferrin analysis and LLO analysis, although a definitive diagnosis can only be achieved through molecular genetic testing. There are currently no approved treatments for ALG12-CDG5.
Synonyms
- CDG-Ig
- Congenital disorder of glycosylation type 1g
Inheritance
ALG12-CDG is an autosomal recessive disorder, meaning an affected individual inherits one defective copy of the gene from each asymptomatic parent.
Gene Function
The ALG12 gene encodes a mannosyltransferase enzyme, alpha-1,6-mannosyltranserase (ALG12). Mannosyltransferases are enzymes that enable the transfer of mannose during glycosylation. ALG12 is a located in the lumen-facing side of ER membrane, where it has a role in the assembly of the LLO, a precursor for protein N-glycosylation. The ALG12 enzyme transfers the eighth of nine mannose residues to the growing N-glycan prior to its attachment to a protein1.
LLO synthesis
N-glycosylation is the process by which an oligosaccharide is attached the nitrogen atom of asparagine residues on proteins. N-glycosylation is initiated in the ER and begins with the synthesis of an LLO14. The LLO is comprised of a 14-sugar oligosaccharide attached to the lipid carrier dolichol pyrophosphate (Dol-PP). The 14-sugar residues are two N-acetylglucosamine, nine mannose, and three glucose resides. Once assembled, the oligosaccharide is transferred “en bloc” to proteins and undergoes further processing in the ER and Golgi14. Once the oligosaccharide is attached to a protein, it is referred to as an N-glycan.
Assembly of the LLO is carried out by a series of enzymes encoded by the ALG genes and can be divided into two phases: Phase I and Phase II (Figure 1)14.
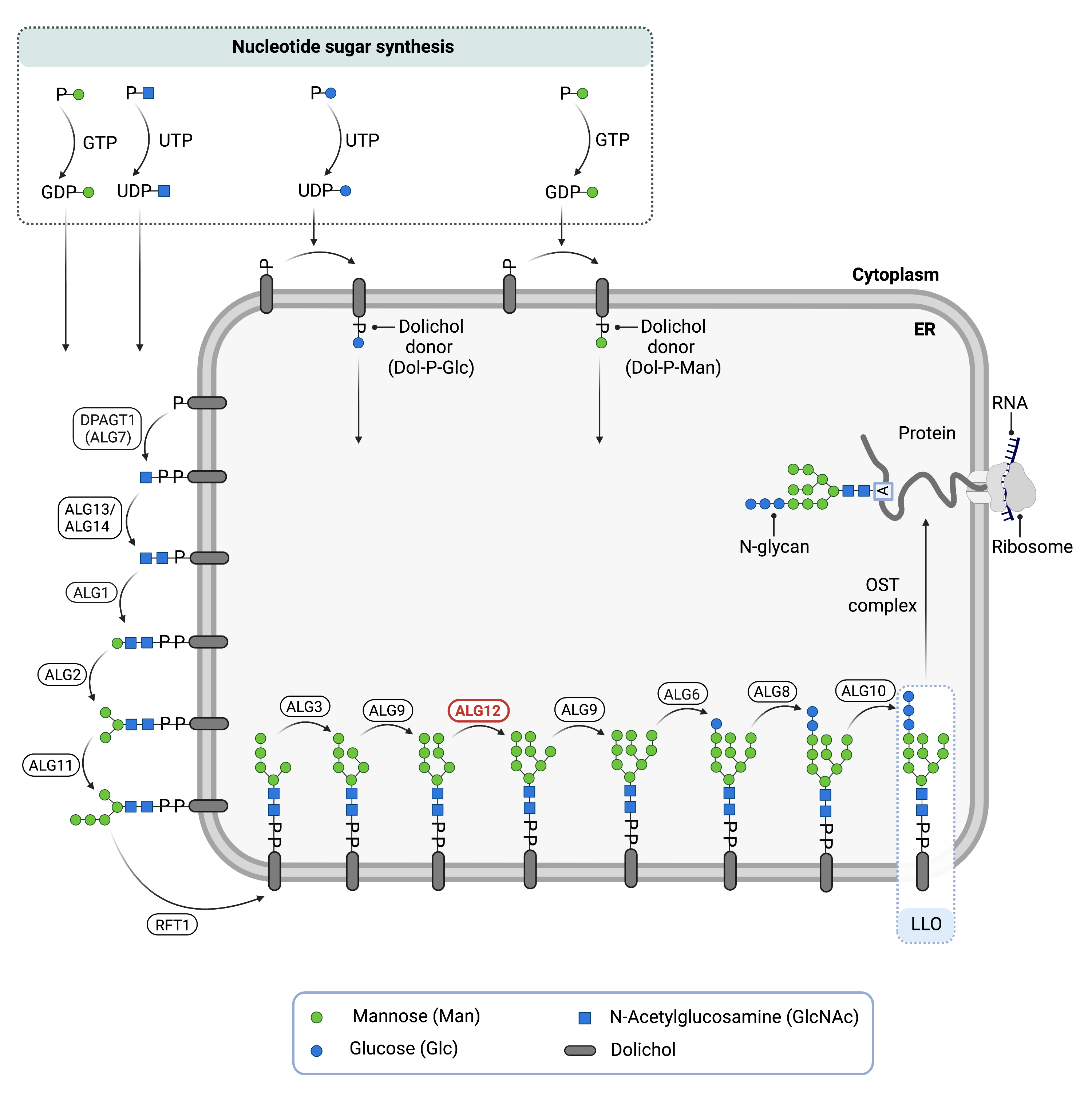
Figure 1. Role of ALG12 in glycosylation.
ALG12 is an enzyme (mannosyltransferase) involved in synthesising the lipid-linked oligosaccharide (LLO), which is needed for N-glycosylation. ALG12 adds a mannose residue to the LLO in the endoplasmic reticulum.
Phase I
Phase I of LLO synthesis takes place on the cytoplasmic side of the ER. It begins with the sequential attachment of two N-Acetylglucosamine (GlcNAc2) and five mannose (Man5) residues to Dol-PP by several ER enzymes. GlcNAc and Man are transferred from nucleotide sugars UDP-GlcNAc and GDP-Man, respectively. The intermediate structure, Dol-PP-Man5GlcNAc2, is translocated across the ER membrane into the lumen via the RFT1 enzyme14,15.
Phase II
Phase II of LLO synthesis takes place in the ER lumen. Once in the lumen, four Man residues followed by three glucose (Glc) residues are added to the intermediate structure, generating the complete the N-glycan, Dol-PP-Glc3Man9GlcNAc2. Man and Glc are transferred from glycosyl donors Dol-P-Man and Dol-P-Glc, which are formed on the cytoplasmic side of the ER and must also be flipped across the ER membrane14. ALG12 is responsible for adding the eighth mannose residue to the growing oligosaccharide chain.
Once assembled, the oligosaccharide is transferred “en bloc” from Dol-PP to an asparagine residue of a newly synthesized protein via the enzyme oligosaccharyltransferase (OST), resulting in N-glycosylation of the protein14. The asparagine residue must be located in regions of the protein where the sequence of amino acids is asparagine-X-serine/threonine, also called Asn-X-Ser/Thr consensus sequence where “X” can be any amino acid except proline. The activity of OST is highly specific for the completely assembled 14-sugar N-glycan, Glc3Man9GlcNAc2.
Disease Mechanism
Mutations in the ALG12 gene lead to the production of an abnormal enzyme with reduced or no activity. In the absence of ALG12, the LLO is missing the eighth and ninth mannose residues and is therefore incompletely assembled. This results in reduced transfer efficiency of the oligosaccharide by OST, resulting in N-glycoproteins that are insufficiently glycosylated (hypoglycosylation)1,16.
Mutations
The ALG12 gene is located on chromosome 22 (22q13.33). To date, 14 pathogenic mutations in ALG12 have been reported5. There are 10 single amino acid substitutions which occur in or near transmembrane domains of the protein, 3 frameshift mutations that result in premature termination of the peptide, and 1 nonsense mutation that gives rise to a stop codon5.
Signs & Symptoms
Clinical Presentation
Individuals with ALG12-CDG develop signs and symptoms that may be detected in infancy or prenatally. ALG12-CDG is primarily characterized by neurological disorder, abnormal features, and recurrent infections. The characteristic clinical presentations of ALG12-CDG include5,13:
- Neurological – intellectual disability, delayed gross motor and speech development, decreased muscle tone (hypotonia), and smaller than average head at birth (progressive microcephaly), and epilepsy
- Dysmorphic features – dysmorphic face (triangular or long), epicanthal folds, abnormal ears, thin upper lip, short philtrum, prominent nasal bridge, broad nose, midface hypoplasia, micrognathia, low posterior hairline with redundant skin, abnormal body fat distribution, and inverted nipples
- Immunologic – recurrent infections of the upper and lower respiratory tracts including ear, nose, and throat, and pulmonary infections are a distinctive feature of ALG12-CDG. B-lymphopenia and impaired antibody response to diptheria, tetanus and Haemophilus influenzae immunizations have been reported, although most patients do not progress to severe infections or sepsis
- Gastrointestinal – feeding difficulties leading to a failure to thrive are common among patients
- Genitourinary – male patients with ALG12-CDG are universally reported with urogenital tract anomalies including micropenis, one or both testes failing to descend into the scrotum (cryptorchidism), and the opening of the urethra is not located at the tip of the penis (hypospadias). There are no reports of abnormalities involving the upper urinary tracts or of the female genital tract
- Cardiac – persistent opening between two major blood vessels leading from the heart (patent ductus arteriosus), muscular intraventricular septal defect, a small opening between the two upper chambers of the heart (patent foramen ovale) and thickening of the heart wall (biventricular hypertrophy) with systolic obliteration of the left ventricular cavity
Other less common symptoms may include ophthalmological abnormalities such as strabismus, retinal detachment, bilateral cataracts, and retinitis pigmentosa, deafness, abnormal brain imaging, and skeletal malformations 5,17.
Biochemical Abnormalities
All ALG12-CDG patients that have been reported in the literature have abnormal coagulation parameters including decreased levels of antithrombin, factor XI, protein C, and protein S, as well as thrombocytopenia. Immune deficiency presentation is associated with decreased levels of immunoglobulins, IgG, IgM, and IgA5.
Classification
ALG12-CDG is classified as a disorder of N-linked protein glycosylation.
Under the former CDG classification system, ALG12-CDG is classified as a Type 1 CDG, which arise due to defects in the synthesis of oligosaccharides or their transfer to proteins.
Diagnosis
Although diagnosis of ALG12-CDG may be suspected based on presentation of symptoms and detailed patient history, direct molecular genetic testing is the only definitive diagnostic test. Screening in suspected patients begins with a blood test to analyze serum transferrin. Lipid-linked oligosaccharide (LLO) analysis in patient fibroblasts may also be carried out following transferrin screening.
Transferrin Analysis
Individuals with ALG12-CDG show a type 1 pattern by transferrin isoelectric focusing (TIEF) or mass spectrometry analysis of transferrin5. Type 1 patterns are observed in CDG that arise due to defects in the N-glycan assembly and are characterized by a decrease in tetrasialo-transferrin and an increase in disialo- and asialo-transferrin isoforms.
Total N-glycan Analysis
N-glycan analysis with matrix-assisted laser desorption/ionization mass spectrometry (MALDI-MS) and electrospray ionization mass spectrometry (ESI-MS) detect an accumulation of aberrant high-mannose and hybrid-glycans, GlcNAc2Man5-7, and decreased levels of GlcNAc2Man8-9 consistent with deficient ALG12 enzyme12,18.
LLO Analysis
LLO analysis of patient fibroblasts show an increase in GlcNAc2Man7 glycans, consistent with ALG12 deficiency5.
Biomarkers
A biomarker that is unique to ALG12-CDG has not been identified.
Prognosis
Prognosis of ALG12-CDG may vary depending on the severity of an individual’s symptoms. As of 2019, the oldest patient reported in the medical literature is 44 years old5. Most patients recorded in the literature are infants or in early childhood, however there are two other patients who have reached adulthood who are 30 years old5 (as of 2019) and 25 years old2 (as of 2020). Severe forms of ALG12-CDG involve developmental delay, vision and hearing impairments, low muscle tone, feeding problems, genital abnormalities, and hypogammaglobulinemia with recurrent infections. Milder cases may have cognitive and coagulation impairments5.
Management
Management of symptoms may include combinations of physical therapy, occupational therapy, speech or vision therapy, and palliative measures.
Some patients with immune deficiency have been treated with scheduled infusions of immunoglobulins5.
Therapies
There are currently no treatment options available for ALG12-CDG. Treatment is focused on management of symptoms and prevention of complications19.
Research Models
Several ALG12 research models have been generated including in yeast, flies, and mice.
Yeast (S. cerevisiae)
Alg12 null mutant yeast have been generated. Mutants show altered sensitivity to a variety of chemicals and have enhanced competitive fitness (YeastGenome).
Fly (D. melanogaster)
Drosophila gene Alg12 (CG8412, FBgn0037743) is orthologous to ALG12, also encodes the alpha-1,6-mannoosyltransferase enzyme. It is a potential model for the human disease ALG12-CDG (FlyBase).
Mouse (M. musculus)
Alg12 conditional-ready floxed knockout embryonic stem cell line
Embryonic stem (ES) cell line Alg6tm1a(EUCOMM)Wtsi is a targeted knockout/null mutation of Alg12. A “conditional-ready” allele can be created by flp recombinase expression in mice carrying this allele, and cre expression results in a knockout mouse. If cre is expressed without flp expression, a reporter knockout mouse can be generated (MGI).
ALG12 knockout ES cell line
ES cell line Alg12tm1e(EUCOMM)Wtsi and Alg12tm1(KOMP)Vlcg are targeted knockout/null mutation of Alg12. Alg12tm1e(EUCOMM)Wtsi uses the L1L2_Bact_P vector (MGI), and Alg12tm1(KOMP)Vlcg uses the ZEN-Ub1 vector (MGI).
Clinical Studies
Active
Clinical and Basic Investigations into Congenital Disorders of Glycosylation (NCT04199000)
The Frontiers in Congenital Disorder of Glycosylation Disorders Consortium (FCDGC) is conducting a 5-year natural history study on all CDG types, including ALG12-CDG. The purpose of this study is to define the natural history and clinical symptoms of CDG, develop new diagnostic techniques, identify clinical biomarkers that can be used in future clinical trials and evaluate whether dietary treatments improve clinical symptoms and quality of life.
Publications
ALG12-CDG Scientific Articles on PubMed
Additional Resources
OMIM
OrphaNet
NORD
GARD
Genetic Testing Registry
ClinVar
NIH
GeneCards
UniProt
FCDGC
References
- Chantret, I. et al. Congenital Disorders of Glycosylation Type Ig Is Defined by a Deficiency in Dolichyl-P-mannose:Man7GlcNAc2-PP-dolichyl Mannosyltransferase. Journal of Biological Chemistry 277, (2002).
- Morena‐Barrio, M. E. et al. ALG12‐CDG: An unusual patient without intellectual disability and facial dysmorphism, and with a novel variant. Molecular Genetics & Genomic Medicine 8, (2020).
- Zdebska, E. et al. Abnormal Glycosylation of Red Cell Membrane Band 3 in the Congenital Disorder of Glycosylation Ig. Pediatric Research 54, (2003).
- THIEL, C. et al. Deficiency of dolichyl-P-Man:Man7GlcNAc2-PP-dolichyl mannosyltransferase causes congenital disorder of glycosylation type Ig. Biochemical Journal 367, (2002).
- Tahata, S., Gunderson, L., Lanpher, B. & Morava, E. Complex phenotypes in ALG12-congenital disorder of glycosylation (ALG12-CDG): Case series and review of the literature. Molecular Genetics and Metabolism 128, (2019).
- Sturiale, L. et al. ALG12-CDG: novel glycophenotype insights endorse the molecular defect. Glycoconjugate Journal 36, (2019).
- Murali, C. et al. Diagnosis of ALG12-CDG by exome sequencing in a case of severe skeletal dysplasia. Molecular Genetics and Metabolism Reports 1, (2014).
- Kranz, C. et al. Expanding spectrum of congenital disorder of glycosylation Ig (CDG-Ig): Sibs with a unique skeletal dysplasia, hypogammaglobulinemia, cardiomyopathy, genital malformations, and early lethality. American Journal of Medical Genetics Part A 143A, (2007).
- Grubenmann, C. E. ALG12 mannosyltransferase defect in congenital disorder of glycosylation type lg. Human Molecular Genetics 11, (2002).
- Eklund, E. A. et al. Molecular and clinical description of the first US patients with congenital disorder of glycosylation Ig☆. Molecular Genetics and Metabolism 84, (2005).
- Rocco, M. di et al. Congenital disorder of glycosylation (CDG) Ig: Report on a patient and review of the literature. Journal of Inherited Metabolic Disease 28, (2005).
- Ziburová, J. et al. A novel homozygous mutation in the human ALG12 gene results in an aberrant profile of oligomannose N-glycans in patient’s serum. Am J Med Genet A 185, 3494–3501 (2021).
- Nicotera, A. G. et al. A Novel Homozygous ALG12 Mutation in a Patient with CDG Type Ig: New Report of a Case with a Mild Phenotype. Mol Syndromol 12, 327–332 (2021).
- Bieberich, E. Synthesis, Processing, and Function of N-glycans in N-glycoproteins. in (2014). doi:10.1007/978-1-4939-1154-7_3.
- Stanley, P., Taniguchi, N. & Aebi, M. N-glycans. in Essentials of Glycobiology [Internet] (eds. Varki, A. et al.) (Cold Spring Harbor Laboratory Press, 2017).
- Ziburová, J. et al. A novel homozygous mutation in the human ALG12 gene results in an aberrant profile of oligomannose N-glycans in patient’s serum. Am J Med Genet A 185, 3494–3501 (2021).
- Esfandiari, H., Mets, M. B., Kim, K. H. & Kurup, S. P. Ocular abnormalities in a patient with congenital disorder of glycosylation type Ig. Ophthalmic Genet 40, 549–552 (2019).
- Hiraide, T. et al. Novel ALG12 variants and hydronephrosis in siblings with impaired N-glycosylation. Brain and Development 43, 945–951 (2021).
- ALG12-congenital disorder of glycosylation (ALG12-CDG, also known as congenital disorder of glycosylation type Ig) | Rare Diseases Clinical Research Network. https://www.rarediseasesnetwork.org/fcdgc/alg12.